
Upper Crossed Syndrome: Anatomy, Adaptation, and the Work of Rebalancing
Upper Crossed Syndrome (UCS) is a common pattern of postural and muscular imbalance involving the head, neck, shoulders, and upper thorax. While often discussed in ergonomic or fitness settings, UCS has particular relevance in osteopathic medicine because it reflects how structure, function, and nervous-system tone influence one another over time.
Rather than being a single diagnosis, UCS describes a pattern—one that frequently accompanies chronic neck pain, headaches, shoulder dysfunction, breathing restriction, and fatigue.
Understanding this pattern allows for practical, effective change.
What Is Upper Crossed Syndrome?
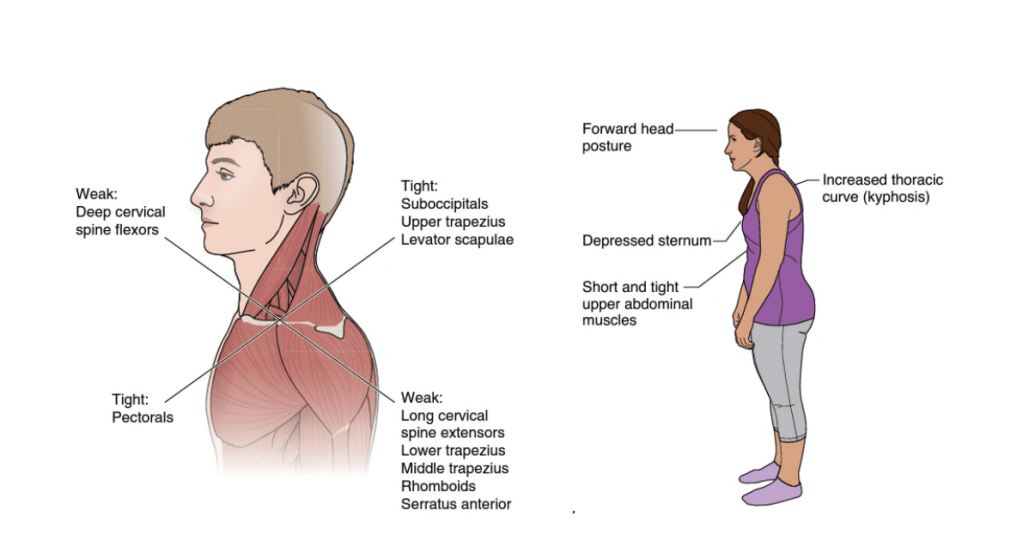
Upper Crossed Syndrome refers to a predictable arrangement of muscular imbalance in the upper body:
- Muscles in the anterior chest and posterior neck/shoulder region tend to become shortened and overactive.
- Muscles responsible for deep neck stabilization and scapular control tend to become lengthened and underactive.
These imbalances “cross” between the front and back of the upper body, creating a characteristic postural presentation: forward head carriage, rounded shoulders, elevated shoulder girdle, and increased thoracic kyphosis.
UCS is biomechanical in expression but systemic in effect.
Key Anatomy Involved
Muscles Commonly Tight or Overactive
- Upper trapezius
- Levator scapulae
- Pectoralis major and minor
- Sternocleidomastoid
- Suboccipital muscles
Muscles Commonly Weak or Inhibited
- Deep cervical flexors (longus colli, longus capitis)
- Middle and lower trapezius
- Rhomboids
- Serratus anterior
- Posterior rotator cuff
The imbalance between these muscle groups alters cervical spine loading, scapular positioning, and shoulder joint stability.
How Upper Crossed Syndrome Develops
UCS most often develops gradually. Contributing factors include:
- Prolonged sitting or screen use
- Sustained forward‑head posture
- Occupations requiring repetitive upper‑extremity work
- Athletic overuse (e.g., swimming, weightlifting without postural balance)
- Previous cervical or shoulder injury
As this posture persists, joint motion changes—particularly at the atlanto‑occipital joint, mid‑cervical spine, cervicothoracic junction, and upper thoracic segments. Rib motion and scapulothoracic mechanics are also affected, altering breathing and upper‑extremity coordination.
Common Symptoms
Because UCS alters multiple regions simultaneously, symptoms are varied and often diffuse:
- Neck pain or stiffness
- Tension‑type headaches
- Shoulder pain or instability
- Upper back discomfort
- Arm tingling or fatigue
- Reduced tolerance for sitting or desk work
- Shallow or restricted breathing
These symptoms frequently overlap with chronic pain presentations and are commonly misunderstood as isolated “neck” or “shoulder” issues.
Why Upper Crossed Syndrome Persists
One reason UCS becomes chronic is that strengthening alone rarely resolves it. When tight muscles remain shortened and joints remain restricted, attempts to “build strength” often reinforce compensation rather than restore balance.
Osteopathic perspectives emphasize that motion must be restored before strength is layered on. Addressing joint restriction, myofascial tone, and breathing mechanics allows muscular retraining to be effective rather than aggravating.
Practical Steps: What the Reader Can Do
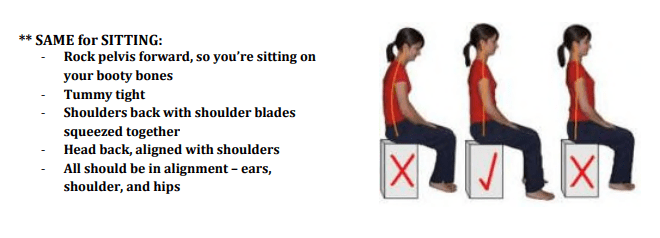
1. Improve Postural Awareness
Begin with awareness, not force. Periodically check head position relative to the torso. A neutral position reduces cervical loading without effort.
2. Mobilize the Thoracic Spine
Gentle thoracic extension exercises (over a rolled towel or foam roller) help counteract excessive kyphosis and improve rib motion, which supports breathing.
3. Lengthen Overactive Muscles
Slow, sustained stretches for the pectoral muscles, levator scapulae, and upper trapezius reduce constant downward and forward pull on the shoulder girdle.
4. Retrain Deep Neck Flexors
Exercises such as small chin‑nod movements (supine or seated) activate deep cervical stabilizers without recruiting larger superficial muscles.
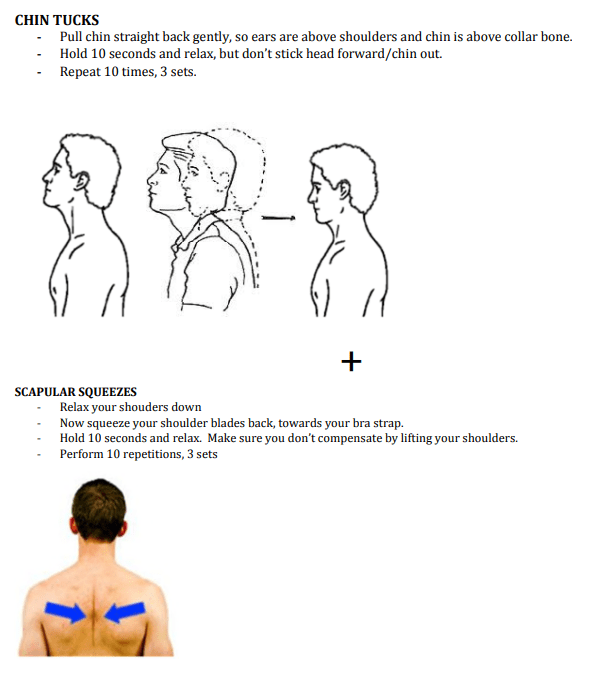
5. Restore Scapular Control
Low‑load exercises emphasizing:
- Serratus anterior engagement
- Lower trapezius activation
- Controlled scapular retraction and depression
should be performed slowly, with attention to symmetry and breathing.
6. Integrate Breathing
Upper chest–dominant breathing is common in UCS. Practicing diaphragmatic breathing with rib expansion supports thoracic mobility and reduces unnecessary neck and shoulder tension. Refer to “Breathe” article on this blogsite for various helpful techniques.
When Osteopathic Care Is Helpful
Osteopathic examination often identifies segmental dysfunction at:
- The atlanto‑occipital junction
- Mid‑cervical spine
- Cervicothoracic junction
- Upper thoracic spine
- Ribs and scapulothoracic interface
Manual treatment addressing these regions can improve joint motion, muscular balance, and fluid dynamics, making exercise and posture correction more sustainable.
Upper Crossed Syndrome and Your Larger Thesis
Within the broader framework of chronic pain and stress‑related conditions, UCS is a visible example of how repeated load and sustained posture reshape the body. Pain does not arise from one muscle acting alone, but from systems that lose variability and coordination.
Addressing UCS successfully means:
- Improving movement options
- Restoring efficient breathing
- Retraining coordination rather than forcing correction
This systems‑based approach aligns closely with osteopathic principles and with modern understandings of chronic pain persistence.
Closing Reflection
Upper Crossed Syndrome is not a personal failure or a simple posture “mistake.” It is a common bodily response to the way many people live and work.
Progress comes not from forcing the body upright, but from restoring balance—segment by segment, breath by breath, movement by movement.
That is where durable change begins.
Primary Reference
- Gorscovoz, V. Osteopathic Amelioration of Upper Crossed Syndrome. National Academy of Osteopathy, 2018. [link.springer.com]
