
Pelvic Pain: Stability, Safety, and the Work of Relearning Movement
Pelvic pain is rarely just a local problem.
For many people living with chronic pain, trauma histories, or prolonged stress, the pelvis becomes a region of protection. Muscles tighten. Motion narrows. Breath avoids depth. Over time, what began as an adaptive response settles into a pattern—one that can quietly sustain pain long after the original trigger has passed.
From an osteopathic perspective, this is entirely logical. The pelvis is a crossroads: spine and legs, viscera and fascia, autonomic nerves and breath. When coordination breaks down here, compensation spreads throughout the body. Addressing pelvic pain therefore means restoring stability without rigidity, and awareness without threat.
Pelvic Stability Is Coordination, Not Force
A common misconception is that pelvic pain reflects weakness alone. In reality, many people with pelvic pain are over‑engaged rather than under‑supported. Muscles such as the pelvic floor, hip flexors, or adductors may grip continuously, while deeper stabilizers fail to coordinate appropriately.
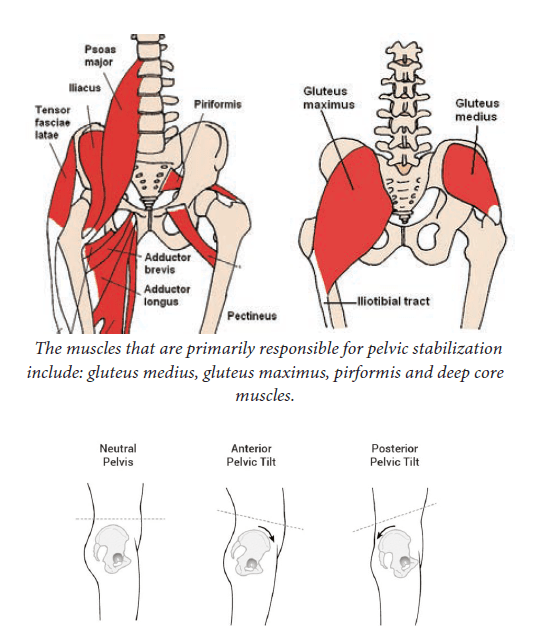
True pelvic stability comes from timing and sequencing, not maximal effort. Muscles like the gluteus medius and deep core should activate smoothly to hold the pelvis neutral as the limbs move. When this system is working, movement feels efficient and safe. When it is not, the body braces—and pain often follows.
A Trauma‑Informed Way to Strengthen
For readers with chronic pain or trauma exposure, how exercises are performed matters more than how difficult they look.
Pelvic rehabilitation works best when movements are:
- Slow and deliberate
- Performed near mid‑range rather than end‑range
- Paired with easy, continuous breathing
- Stopped if pain escalates or lingers
This approach reduces threat signaling to the nervous system and allows the brain to relearn movement patterns. Pain decreases not because the body has been forced to comply, but because it no longer feels the need to protect.
Foundational Movements That Support the Pelvis
Certain movement patterns are particularly useful when rebuilding pelvic control.
Posterior‑chain activities like gentle bridges help reintegrate the hips and pelvis, especially when attention is placed on using the gluteal muscles rather than the low back or hamstrings. Side‑lying hip work builds lateral stability, which is essential for walking and standing without strain.
Single‑leg variations introduce controlled asymmetry. Life is asymmetric; training should be too. These movements teach the pelvis how to remain stable while weight shifts—something often lost in chronic pain states.
Progression matters. Stability should improve before load increases.
Pelvic Pain and Biofeedback
For individuals who have difficulty sensing pelvic movement—or for those with pelvic floor pain, incontinence, or sexual pain—pelvic biofeedback can be a helpful adjunct.
Devices such as Perifit provide real‑time feedback that helps users learn when they are contracting, relaxing, or over‑recruiting. The most therapeutic use of these tools emphasizes awareness and relaxation, not constant tightening.
This is especially important in trauma‑related pelvic pain, where symptoms are frequently driven by persistent overactivity rather than weakness. Biofeedback becomes a way to listen, not dominate.
Breath and the Pelvis
Pelvic stability cannot be separated from breathing.
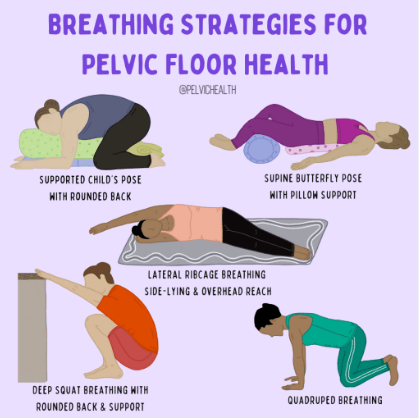
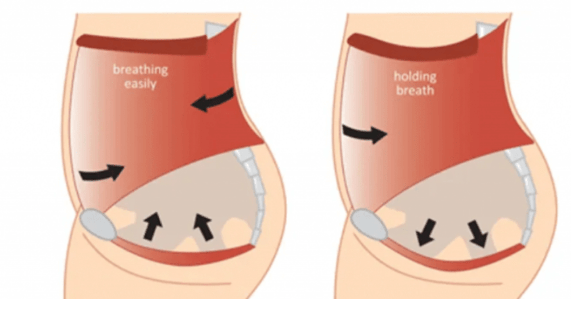
The diaphragm, abdominal wall, and pelvic floor form a functional unit. When breath is shallow or held, pelvic tone often increases. When breathing is slow and expansive, pelvic tissues tend to soften.
During movement and exercise:
- Allow the inhale to widen the ribs and belly
- Let the exhale descend naturally into the pelvis
- Avoid breath holding during effort
This pairing reinforces parasympathetic activity and supports the nervous system’s ability to down‑regulate while moving.
When Hands‑On Care Matters
Some patterns are difficult to change through exercise alone. Persistent pelvic pain—especially after childbirth, surgery, trauma, or long‑standing dysfunction—often benefits from manual assessment and treatment.
Osteopathic evaluation can address restrictions in the sacrum, lumbar spine, hips, diaphragm, and pelvic floor, as well as visceral and fascial relationships that influence pelvic mechanics. Pelvic floor physical therapy can add targeted rehabilitation and biofeedback when indicated.
The most effective care is often integrative, not singular.
Pelvic Pain in the Larger Picture
Within the larger framework of this blog, pelvic pain represents a convergence point. It reflects how chronic pain, trauma, and nervous‑system dysregulation manifest in the body.
Healing here is not about “fixing” a broken structure. It is about restoring adaptability—teaching the pelvis and nervous system that movement can occur without danger.
When stability and safety return together, pain often loosens its hold.
Closing Reflection
Pelvic pain does not mean something is wrong with you.
Often, it means your body has been protecting something important for a very long time.
Stability is not clenching.
Strength is not force.
Healing is the slow return of choice.
When movement feels safe again, the pelvis can shift from a place of defense back into a foundation for living.
Further Reading & Study
Osteopathy‑Focused Texts
- Fulford, R.C. Dr. Fulford’s Touch of Life – Broader context for resonance, motion, and vitality
- Barral, J‑P. Urogenital Manipulation – Visceral approaches to pelvic and urogenital dysfunction
- Sandler, S. Osteopathy and Obstetrics – Comprehensive coverage of pelvic, cranial, and visceral care
- Bayliss, J.R. The Pelvic Book for Osteopaths and Chiropractors – Manual techniques and clinical reasoning
- A Manual of Osteopathic Gynecology – Classical osteopathic perspectives on pelvic anatomy and disease
Patient‑Focused / Anatomy Books
- Calais‑Germain, B. The Female Pelvis: Anatomy & Exercises – Clear anatomical understanding and movement
- Reardon, S. Floored – Accessible guidance on pelvic floor dysfunction for the general public
