
Temporomandibular disorders (TMD) are common, frequently missed, and often misunderstood.
Many patients are told their symptoms are “stress,” “anxiety,” or “just clenching.” Others receive treatments that quiet symptoms temporarily but make the problem worse over time. Yet from an osteopathic perspective, uncomplicated TMJ dysfunction is often quite treatable—when we understand why the jaw is behaving the way it is.
The jaw is not an isolated joint.
It is a crossroads of posture, breath, nervous system tone, and lived experience.
Why TMJ Is Often Misdiagnosed
The temporomandibular joint sits at the intersection of the cranium, face, cervical spine, and upper airway. Pain here can radiate into the teeth, face, ears, head, neck, shoulders, or behind the eyes. Symptoms may include clicking or popping, stiffness, facial swelling, tinnitus, headaches, or a sense of jaw instability.
Because the symptoms are so varied, TMJ dysfunction is frequently treated as a dental problem alone—or dismissed entirely. Traditional approaches that aim only to suppress movement, immobilize the jaw, or permanently alter bite mechanics can reduce symptoms short term while increasing long‑term rigidity.
In chronic pain, rigidity is rarely the answer.
The Jaw as a Stress Barometer
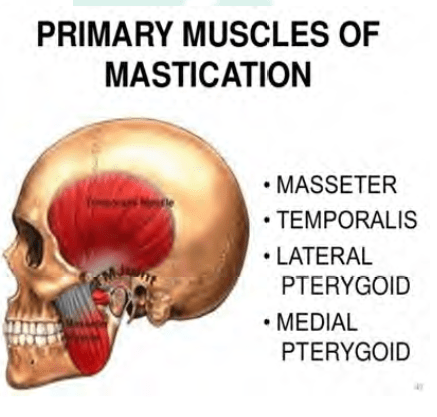
Clenching, grinding, and jaw holding are among the most common human stress responses. The muscles of mastication—masseter, temporalis, pterygoids—are powerful, fast to react, and deeply connected to threat physiology.
From a nervous‑system perspective, the jaw is one of the first places protection appears.
This helps explain why TMJ dysfunction is often associated with:
- Anxiety
- Trauma history
- Sleep disturbance
- Headaches or migraines
- Chronic neck or shoulder pain
And why it disproportionately affects women, particularly in early adulthood—a time when cranial, sacral, and hormonal systems are still settling into adult patterns.
Osteopathic Biomechanics: What Goes Wrong
Normal jaw movement involves a smooth sequence:
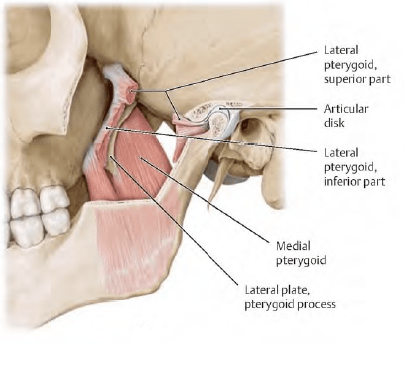
- Initial rotation of the mandibular condyles
- Followed by anterior glide as the disc and condyle move together
The lateral pterygoid muscle plays a critical role in guiding the articular disc. When this muscle is chronically tense—often due to postural strain, dental procedures, trauma, or stress—the disc may be pulled forward.
This is where clicking and popping come from.
In many cases:
- The disc sits anterior to the condyle at rest
- On opening, the disc reduces suddenly (click)
- On closing, it may slip forward again (click)
If reduction no longer occurs, the jaw may feel stuck or unable to open fully—a “closed lock.”
Importantly, the problem is rarely just the disc.
It is abnormal tension and coordination in the system.
TMJ and Trauma: A Shared Language
Trauma does not only live in memories.
It lives in tone, posture, and reflex.
The jaw, like the pelvis, is a region where survival responses accumulate. Holding the mouth closed, clenching the teeth, bracing the neck—these are protective strategies. Over time, they stop being voluntary.
Chronic jaw tension becomes a baseline state.
Approaching TMJ purely as a mechanical failure misses this entirely.
Practical Steps: What the Reader Can Do
1. Start With Awareness, Not Strength
Notice your resting jaw position. Lips together. Teeth apart. Tongue resting lightly against the palate. This resting posture alone often reduces symptoms over time.
2. Reduce Global Threat
Jaw tension increases when the nervous system is activated. Slow breathing—especially longer exhales—can reduce masseter and temporalis tone surprisingly quickly.
A simple check: if your jaw feels tense, your breath likely is too.
3. Gentle Jaw Mobility (Pain‑Free Range Only)
Instead of forcing wide opening, practice:
- Small, slow opening and closing
- Focus on symmetry
- Stop before clicking when possible
The goal is restoring coordination, not stretching aggressively.
4. Address the Neck and Upper Back
TMJ dysfunction often improves when cervical spine mobility, posture, and scapular stability improve. The jaw follows the head.
5. Avoid Habitual Over‑Stretching
Forceful stretching, excessive gum chewing, wide yawning, or aggressive massage can worsen disc mechanics. More is not better.
When Additional Support Helps
Osteopathic treatment can address:
- Cranial strain patterns
- Temporomandibular ligaments
- Cervical and upper thoracic mechanics
- Fascial continuity between jaw, neck, and breath
Other adjuncts may include:
- Thoughtfully designed dental splints (not all splints are equal)
- Physical therapy focused on motor control, not bracing
- Appliances such as ALF in selected cases
- In refractory cases, prolotherapy or regenerative approaches
Surgery is rarely first‑line and often unnecessary.
TMJ in the Larger Picture
TMJ dysfunction is not “just a jaw issue.” It is a window into how the body responds to sustained stress and unresolved threat.
Like chronic pelvic pain or low back pain, it reflects a system that has learned to hold on.
The work is not to force release.
It is to restore safety, coordination, and adaptive movement.
When the nervous system feels safe enough, the jaw often softens on its own.
Closing Reflection
The jaw speaks even when we do not.
It clenches when words are swallowed.
It braces when danger is anticipated.
TMJ pain is not a failure of anatomy.
It is often a history written in muscle and motion.
Listen to it carefully—with hands, with breath, and with respect—and it may no longer need to shout.
